Foamy Urine: What It Means and When to See a Doctor
Many people may have experienced going to the bathroom and noticing that their urine looks unusually foamy or bubbly. While it might be alarming at first, foamy urine is a relatively common occurrence. In most cases, it’s nothing to worry about, but in some situations, it could be a sign of an underlying health issue. It’s important to understand what causes foamy urine and what actions should be taken if it is noticed.
What Causes Foamy Urine?
In most cases foamy urine is nothing to worry about, but in some situations, it could be a sign of an underlying health issue.
There are several reasons why urine might appear foamy:
Dehydration
When a person isn’t drinking enough fluids, their urine becomes more concentrated. This can cause it to appear darker and foamier than usual. The foam is caused by the higher concentration of proteins and other compounds in the urine.
Rapid urination
If someone has a full bladder and urinates with a lot of force, the stream can create bubbles in the toilet bowl. This is a normal occurrence and not a cause for concern.
Cleaning products
Sometimes, residual cleaning products in the toilet bowl can react with urine and create foam. This is not related to a person’s health.
Kidney disease
In some cases, foamy urine can be a sign of kidney disease. When the kidneys are damaged, they can allow protein to leak into the urine, causing it to appear foamy. This condition, known as proteinuria, can be an early sign of kidney dysfunction.
Diabetes
High blood sugar levels can cause the kidneys to work harder, potentially leading to kidney damage and protein leakage into the urine. In fact, moderately increased albuminuria (microalbuminuria) is often one of the first signs of diabetic kidney disease.
Certain medications Some medications, such as those used to treat hypertension (ACE inhibitors and ARBs), can cause proteinuria as a side effect.
While not a common cause of foamy urine, UTIs can sometimes lead to excess protein in the urine due to inflammation.
Other Factors Affecting Urine Foam
Interestingly, the composition of urine itself can contribute to foam formation. A recent study published in the Clinical Journal of the American Society of Nephrology discussed how certain organic compounds called surfactants, which are naturally present in urine, can cause bubbling. These surfactants have both hydrophilic and hydrophobic ends, allowing them to trap pockets of air and create bubbles.
The researchers found 16 metabolites with surfactant properties in normal human urine, mostly bile salts and fatty acid esters. In some conditions, such as liver disease (cholestasis) or small intestinal bacterial overgrowth, these metabolites may be present in higher than usual amounts, potentially leading to foamy urine even in the absence of proteinuria.
When to See a Doctor About Foamy Urine
If a person notices foamy urine frequently, especially if it’s accompanied by other symptoms, it’s a good idea for them to see a doctor.
If a person notices foamy urine frequently, especially if it’s accompanied by other symptoms like swelling in the legs or around the eyes, it’s a good idea for them to see a doctor. The doctor can run some simple tests to check kidney function and rule out any underlying health issues.
The doctor will likely start with a urine dipstick test, which can detect the presence of protein in the urine. If the test comes back positive, they may recommend additional tests, such as a 24-hour urine collection, to get a more accurate measure of the amount of protein being excreted. In some cases, the doctor may also recommend imaging tests like an ultrasound or CT scan to get a better look at the kidneys and check for any structural issues.
What to Do About Foamy Urine
If foamy urine is caused by dehydration, the solution is simple: the person should drink more fluids! They should aim for at least 8 glasses of water per day, and more if exercising or spending time in hot weather.
If an underlying health condition is causing the foamy urine, treatment will depend on the specific issue. For example, if a person has diabetes, managing blood sugar levels through diet, exercise, and medication can help protect the kidneys and reduce protein leakage.
If kidney disease is the culprit, the doctor may recommend medications to help control blood pressure and slow the progression of the disease. In some cases, lifestyle changes like eating a low-sodium diet and getting regular exercise can also help.
It’s important to note that while foamy urine can be a sign of kidney problems, not all cases of proteinuria indicate significant kidney damage. Isolated proteinuria (protein in the urine without other signs of kidney dysfunction) is often benign and may not require extensive evaluation. However, if proteinuria is persistent or associated with other concerning symptoms, further workup is warranted.
The Bottom Line
Foamy urine is often harmless, but it can sometimes be a sign of an underlying health issue like kidney disease or diabetes. If a person notices foamy urine frequently, especially if it’s accompanied by other symptoms, it’s a good idea for them to see their doctor for an evaluation. With prompt treatment, many of the conditions that cause foamy urine can be managed effectively.
People should pay attention to the clues their urine provides about their overall health, and it’s always better to err on the side of caution when it comes to protecting the kidneys.
When seeing a urologist for erectile dysfunction (ED), many men ask about oral medications (pills that can be taken by mouth).
These drugs have been a major force in erectile dysfunction treatment for over two decades. Sildenafil (brand name Viagra®) was the first to be approved by the U.S. Food and Drug Administration (FDA) in 1998. Tadalafil (Cialis®) and vardenafil (Levitra®) followed; both drugs were approved in 2003. The FDA approved the fourth ED drug, avanafil (Stendra®) in 2012.
All of the drugs are classified as phosphodiesterase type 5 (PDE5) inhibitors, and they work in similar ways. Many men find them effective and convenient.
Still, they’re not right for every man, and there are differences among them that men should be aware of.
How do oral ED drugs work?
There are differences among oral medications for ED that men should be aware of.
For a man to get an erection, muscles in the penis need to relax so that blood can flow in during sexual stimulation. As the penis fills with blood, it becomes firm and erect. A chemical called nitric oxide, which is naturally produced by the body, helps this process along.
The four oral ED drugs help nitric oxide do its job so that the penis muscles can relax and let the blood in.
ED drugs do not create an erection automatically, however. A man still needs sexual stimulation to achieve an erection.
How are oral ED drugs similar?
Oral ED drugs share these similarities:
In the United States, they are available by prescription only.
ED drugs are not sold over the counter, and men need a doctor’s prescription to obtain them.
It’s important for men to see a doctor when they start having trouble with erections. ED can be a sign of health conditions like diabetes and heart disease. If these conditions are found, they can be treated along with the ED.
ED can be a sign of health conditions like diabetes and heart disease.
ED drugs don’t increase sexual desire.
ED drugs allow blood to flow into the penis more easily to create an erection, but they do not affect sexual desire. Men need to have the drive for sexual activity as well as sexual stimulation for the drugs to work.
ED drugs don’t prevent pregnancy or lower risk for sexually transmitted infections.
Couples still need to use contraceptives and follow safe sex practices, like using condoms and dental dams.
ED drugs have some side effects in common.
The 4 ED drugs do share some mild side effects, such as headache and flushing.
They also have some more serious side effects in common. If any of these symptoms occur, patients should seek emergency medical care:
An erection lasting longer than 4 hours
Sudden loss of vision
Sudden loss of hearing
Ringing in the ears
Dizziness
Swelling of the face, mouth, throat, hands, feet, or legs
However, other side effects may be different for each drug:
Avanafil
Mild side effect:
Back pain
Side effects that need emergency care:
Rash
Itching
Sildenafil
Mild side effects:
Heartburn
Diarrhea
Nausea
Nosebleeds
Numbness or tingling in the limbs, hands, or feet
Pain in muscles, back, or limbs
Changes in color vision, such as a blue tinge or trouble seeing the difference between blue and green
Sensitivity to light
Nasal congestion
Side effects that need emergency care:
Blurred vision
Fainting
Chest pain
Shortness of breath
Rash, itching or hives
Difficulty breathing or swallowing
Tadalafil
Mild side effects:
Heartburn
Nausea
Diarrhea
Pain in the muscles, back, arms, legs, or stomach
Coughing
Side effects that need emergency care:
Blurry vision
Changes in color vision, such as a blue tinge or trouble seeing the difference between blue and green
Chest pain
Hives, rash, blisters, or peeling skin
Difficulty breathing or swallowing
Vardenafil
Mild side effects:
Nausea
Heartburn
Stuffy or runny nose
Flu-like symptoms
Side effects that need emergency care:
Blurry vision
Changes in color vision, such as a blue tinge or trouble seeing the difference between blue and green
Hoarseness
Difficulty breathing or swallowing
Fainting
Hives or rash
Patients should note that some side effects are more common with specific drugs. For example, men who take sildenafil may be more likely to experience a blue/green tinge to their vision than men who take tadalafil. And men who take tadalafil may be more likely to have muscle pain (myalgia) than men who take sildenafil.
A man’s doctor can best advise on the likelihood of certain side effects and how they might affect a man’s personal situation.
ED drugs are not safe for all men.
Men who take drugs containing nitrates should not take ED medications. This combination can cause a dangerous drop in blood pressure. Some examples of nitrates are nitroglycerin, isosorbide mononitrate, and isosorbide dinitrate. Nitrates are prescribed to prevent or treat chest pain related to heart disease.
ED drugs are also not appropriate for men with low blood pressure, uncontrolled high blood pressure, and severe liver disease. Men who are on dialysis for kidney disease should also not take ED drugs.
Men who take alpha blockers for enlarged prostate symptoms may need to space out their doses of these drugs and ED drugs to avoid an interaction.
Men should always tell their doctor about any other medications, street drugs, herbs, or supplements they use. These products may interact with ED drugs.
In addition, men should let their doctor know if they typically eat grapefruit or drink grapefruit juice, as this combination may cause an interaction as well.
How are oral ED drugs different?
Dosing may be different.
Sildenafil, avanafil, and vardenafil are taken on an as-needed basis, meaning a man takes them before he wishes to have an erection. Tadalafil may also be taken this way, but some prescriptions call for it to be taken every day. Men should be sure to take their medicine as directed.
The time between taking the drug and getting an erection may vary.
ED drugs do not produce an erection immediately. It takes some time for the drug to work, and these time frames vary by medication. For example, men usually get an erection about 30 to 60 minutes after taking sildenafil or vardenafil. Men who take tadalafil as needed (not daily) may need to wait 30 to 45 minutes. For those who take avanafil, the wait may be 15 to 30 minutes.
They last for different durations.
ED medications also vary in how long they are effective. For example, once sildenafil or vardenafil take effect, a man might be able to get an erection for four to five hours. For avanafil users, the time frame is about six to twelve hours. Tadalafil has the longest effective time—usually 24 to 36 hours for as- needed users. Men who take tadalafil daily should be able to get an erection at any time.
Which ED drug should a man choose?
When prescribing ED drugs, doctors take many factors into account. They consider a man’s overall health and the drugs and supplements he currently takes.
Sometimes, it takes time to find the most effective ED drug. These medications have been shown to be quite effective, but results vary from man to man. If a particular drug doesn’t work as well or has bothersome side effects, a man’s doctor may prescribe a different drug or suggest a different ED treatment.
It’s important to remember that in the United States, ED drugs are available only by prescription. Men may see online advertisements for non-prescription products that claim to improve erectile function. But these claims are often misleading, and taking such products could be dangerous. (Learn more about sexual enhancement supplements here.)
Genitourinary Syndrome of Menopause (GSM), formerly known as vulvovaginal atrophy (VVA) or atrophic vaginitis, is a common condition that affects many women during and after menopause. It is primarily caused by the hormonal changes that occur during menopause, specifically the decline in estrogen levels. Estrogen plays a crucial role in maintaining the health of the genital and urinary tissues in women.
What are the symptoms of Genitourinary Syndrome of Menopause?
GSM encompasses a range of symptoms and changes in the genital and urinary tract, including:
Vaginal dryness: Reduced estrogen levels can lead to a decrease in vaginal lubrication, making sexual intercourse uncomfortable or painful.
Vaginal atrophy: The vaginal walls become thinner, less elastic, and more fragile, which can cause itching, burning, and discomfort.
Genital discomfort: Women with GSM may experience pain, soreness, or a sense of irritation around the vulva.
Dyspareunia: Painful sexual intercourse is a common symptom of GSM due to the thinning and dryness of the vaginal tissues.
Urinary symptoms: Some women with GSM may experience urinary problems, such as urinary urgency, frequency, or recurrent urinary tract infections, as the tissues in the urinary tract also become affected by the estrogen deficiency.
Recurrent urinary tract infections: Changes in the urinary tract can make women more susceptible to urinary tract infections.
Treatment for Genitourinary Syndrome of Menopause
GSM treatment typically involves the use of estrogen therapy, which can be administered in various forms, including vaginal creams, tablets, rings, or patches. These treatments can help restore the thickness and elasticity of the vaginal tissues and alleviate many of the associated symptoms.
Additionally, pelvic floor muscle training, lubricants, moisturizers, selective estrogen receptor modulators, vaginal DHEA and vaginal vibratory devices may also aid in the therapy.
Is Vaginal Estrogen Safe?
The use of vaginal estrogen therapy for the treatment of Genitourinary Syndrome of Menopause (GSM) is generally considered safe and effective when used as prescribed and under the guidance of a healthcare provider. However, as with any medical treatment, there are potential risks and benefits to consider.
Here are some key points to keep in mind regarding the safety of vaginal estrogen therapy:
1. Localized Treatment: Vaginal estrogen therapy is a localized treatment, meaning it primarily affects the vaginal and urinary tissues. The estrogen is absorbed in smaller amounts compared to systemic (whole-body) hormone replacement therapy (HRT), which minimizes the risk of some systemic side effects.
2. Effectiveness: Vaginal estrogen therapy is highly effective at relieving the symptoms of GSM, such as vaginal dryness, atrophy, and discomfort, as it helps restore the health of the vaginal and urinary tissues.
3. Low Absorption: When used as directed, vaginal estrogen preparations have minimal absorption into the bloodstream. This reduces the risk of systemic side effects associated with estrogen therapy.
4. Minimal Systemic Effects: While systemic estrogen therapy (like a pill or pellets under the skin) may have potential risks like an increased risk of blood clots, breast cancer, and cardiovascular issues, these risks are eliminated with vaginal estrogen because of the lower systemic absorption.
The latest study published in 2023 looking at a large group of women with previous history of breast cancer, the use of vaginal estrogen did NOT increase their risk of cancer recurrence.1
Erectile Dysfunction: Coping Before and During Treatment
Erectile dysfunction (ED) – difficulty with erections – is quite common. In fact, an estimated 30 million men in the United States have ED to some extent. Some men are unable to get an erection at all. Others may get an erection, but it’s not firm enough for sex.
No matter what causes it or how it develops, ED can affect a man’s well-being and his ability to enjoy sex. Men may question their masculinity and their ability to satisfy a sexual partner. They may become anxious about sex and worry about their performance. And they may feel sad about changes to a once-active sex life.
There is good news, however. Over the years, scientists have developed several effective treatment approaches, including lifestyle changes, pills, injections, vacuum devices, suppositories, and penile implant procedures.
Still, it can take a little time to find the right treatment. And with lifestyle changes and surgery, it takes time for the situation to improve. What can men do in the meantime? How can they cope with ED in the here and now?
Read on to find out.
Learn about ED
Over the years, scientists have developed several effective treatment approaches
Learning as much as possible about ED is a useful starting point. A man’s doctor can recommend reliable websites, brochures, podcasts, videos, books, and magazines for learning more. Asking questions while seeing the doctor is another opportunity. Some men write out their questions before their appointment so they don’t forget them.
For example, men might ask:
What’s causing my ED? What can I do about it?
What treatment options are available to me?
Are treatments covered by insurance?
Do you think sex therapy would help me?
Once men have some background knowledge, they can come up with a treatment plan with their doctor.
Communicate with partners
Some people shy away from talking about sex. But being open and honest about ED is an important part of coping – for both partners.
Such discussions allow couples to better understand each other’s point of view. One partner may not be aware of how the other is feeling.
For example, if the man with ED starts avoiding sex, his partner might worry that they are not attractive or fulfilling his needs. And that might not be the case at all.
Having these conversations allow partners to comfort, reassure, and encourage each other. Couples who need help with their communication skills might consider counseling.
Redefine intimacy
There is more to intimacy than penetrative intercourse, and couples can maintain their intimate bond in other ways. Doing so can be as simple as holding hands at the mall, cuddling on the couch during a movie, or giving each other a massage at the end of a long day. In the bedroom, it can be having oral sex or role playing a favorite fantasy.
This is a time to experiment, relax, and have fun. Couples may discover new activities they enjoy – activities that they continue after erections improve. Some see a sex therapist for new ideas, perspectives, and communication tips.
Stay healthy
Eat nutritious foods. Exercise regularly. Quit smoking. Get enough sleep. Practice self-care. These suggestions often top lists of recommended healthy habits. They help with erections, too.
For example, healthy habits lower the risk of health conditions like diabetes and heart disease, which can lead to ED. Research suggests that following a Mediterranean diet could be good for erections, too.
Staying fit and maintaining a healthy weight boosts confidence and body image. It may also improve depression or anxiety that often accompany ED. Read more about lifestyle changes and ED here.
Celebrate successes
Even if ED is frustrating, treatment offers many reasons to celebrate:
Making a first appointment with a urologist
Talking about sex with a partner
Trying a new way of intimacy
Trying a new treatment
Seeing a counselor or sex therapist
Eating healthier meals for a week
Sticking to a workout routine
Making a plan to quit smoking.
Getting a firmer erection than last time
No matter how small an achievement may seem, celebrating progress can boost motivation, confidence, and hope for the future. How men celebrate is up to them. Having date night with their partner, playing a round of golf, or seeing a favorite band can all work.
Stay in touch with a doctor
As noted above, ED treatment can take time. What works well for one man might not be so effective for another. That’s why it’s important for men to stay in touch with their doctor throughout the process. If one approach doesn’t seem to work, there are others to try. Keeping the doctor informed can help them tailor treatment.
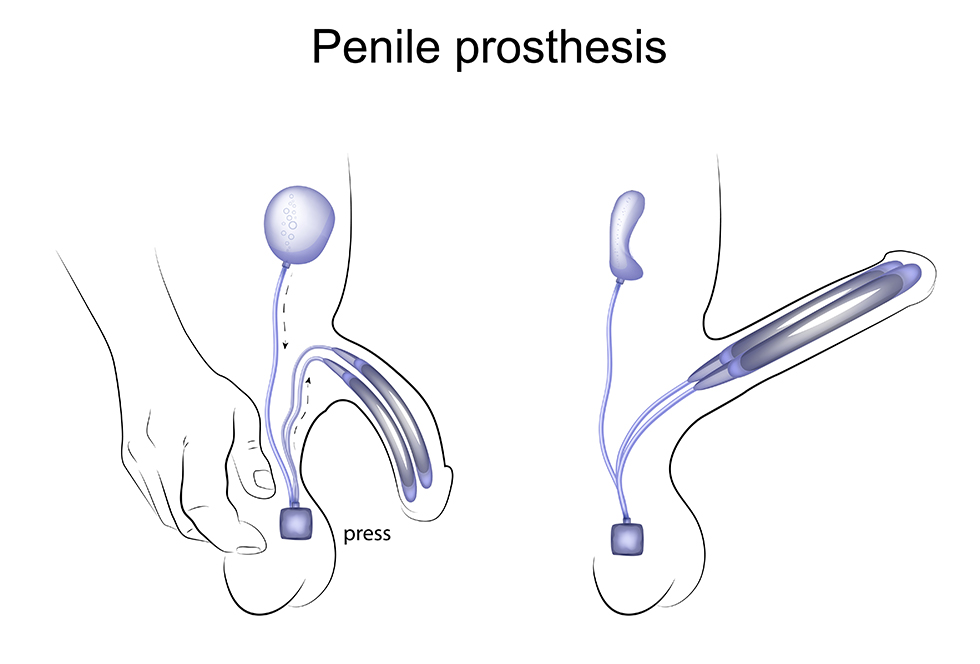
A penile implant (also called a penile prosthesis) is a surgically placed, mechanical device that helps a man get an erection—and keep it—for as long as he likes. It’s one of several treatment options for men with erectile dysfunction (ED). And it has high satisfaction rates.
Still, men need to weigh some important pros and cons before getting an implant. Read on to learn more about the different types of implants, the surgery involved, and what men can expect afterward.
Why do men choose penile implants?
Erectile dysfunction—the inability to get an erection firm enough for sex—is a common problem. While there are several treatments available, such as pills, self-injections, and vacuum devices, they’re not suitable for all men. For example, men who take nitrates for heart conditions cannot use ED medications because of a dangerous drug interaction.
Success with ED treatments can vary, too. What works for one man may not work for another. Generally, men try other ED treatment options before deciding on an implant.
Men with Peyronie’s disease may also get penile implants. This condition causes the penis to bend, sometimes to a point where intercourse becomes quite difficult. An implant can straighten the penis and help with any erection problems.
Transgender men may get penile implants as they undergo gender affirmation surgeries. During these procedures, surgeons create a penis and may implant a prosthesis to aid sexual activity.
Types of penile implants
In general, there are two different types of implants:
Inflatable implants
The most common type of implant is a 3-piece inflatable implant. The three parts are connected by tubes. They include:
A pair of inflatable cylinders that are inserted into the shaft of the penis
A fluid-filled reservoir placed in the abdomen
A pump placed in the scrotum
When a man wishes to have an erection, he simply activates the pump in his scrotum. Saline fluid from the reservoir then moves into the cylinders and inflates them, creating the erection. When the man is done with sexual activity, he presses on the pump again. The cylinders deflate and the fluid moves back to the reservoir.
A 2-piece inflatable implant is also available, but it’s less common. This type works in a similar way, but the reservoir and the pump are in the same piece.
Malleable (semirigid) implants
These implants are flexible silicone rods that are inserted into the penis. When a man wants an erection, he can simply lift his penis up into position, then move it back down when he is finished with sexual activity. Malleable implants are not common nowadays, but they might be suitable for men who may have trouble activating a pump in the scrotum.
Advantages of penile implants
The man has full control. A man can get an erection and keep its firmness for as long as he likes. He can also have as many erections in a day as he wishes.
They have high satisfaction rates. Studies have shown that the satisfaction rate among men with 3-piece implants is 90% or higher.
Sex can be more spontaneous. A man does not have to worry about timing the dose of a pill or stopping sexual activity to give himself an injection or use a vacuum device. Instead, he can create an erection in the moment.
Implants last for years. Some men get 15 to 20 years of use from the same implant before it needs replacing.
They’re discreet. The penis looks natural. People usually can’t tell if a man has an implant by looking at his penis. (Malleable implants may be an exception, as the penis is always somewhat firm.) During intercourse, partners usually cannot tell that a man has an implant.
They don’t affect sexual desire or performance. For most men, sexual sensations, ejaculation, and orgasms feel the same as they did before the implant.
They may boost a man’s sexual confidence. Men may feel less anxious about intimacy knowing that they can get a firm erection every time they have intercourse.
A man can get an erection and keep its firmness for as long as he likes.
Disadvantages of penile implants
A surgical procedure is involved. Like any surgery, penile implant surgery has risks, such as infection, bleeding, and injury to surrounding areas. However, surgeons take special precautions to lower the risk of complications. Infection rates are estimated to be 1% to 2%. If there is an infection, the device is usually replaced.
Implants can malfunction. There are times when a penile implant can malfunction, although this is rare.
They are permanent. Because of the nature of implant surgery, a man can no longer have natural erections once he has an implant. Other ED treatments, such as pills or injections, will no longer be options.
What happens during penile implant surgery?
Before surgery, a man’s doctor will tell him how to prepare. The man may receive special instructions for taking medications or supplements, eating and drinking, and bathing beforehand.
The surgery itself is performed under general anesthesia and takes about one to two hours. It may be done as an outpatient procedure, and many men can go home the same day. However, some men may need to spend a night in the hospital.
To implant the device, the surgeon makes a small incision in the genital area. The inflatable cylinders (or bendable rods, if a malleable implant) are inserted into the shaft of the penis. If it is a 3-piece inflatable device, small incisions are made so that the reservoir can be placed in the abdomen and the pump can be placed in the scrotum. The pieces are then connected and the incisions are closed. The man may have a temporary surgical drain.
Men having implant surgery will need to have someone drive them home. They should also have someone stay with them for the first day or two.
Note: Not all men are good candidates for implant surgery. Men who are at higher risk for complications and those who have heart disease or poorly managed diabetes may not be able to have surgery.
Recovering from penile implant surgery
Back at home, men recovering from implant surgery may experience swelling, pain, or discomfort for the first week. These symptoms may be managed with medicines and ice packs. If there is a drain, it will be removed in the first few days after the procedure.
Men will need to avoid heavy lifting and vigorous activity, including exercise, for up to four weeks. If they work a desk job, they can return to work after a week or so. Men with more physical jobs may need to wait up to four weeks before returning to work.
Sex—both intercourse and masturbation—will need to wait four to six weeks while the body heals. At this time, the man’s doctor will teach him how to use the implant.
Men who have the following symptoms during recovery should call their doctor right away:
Heavy bleeding
Fever
Worsening pain
Infection
Adjusting to a penile implant
It may take time to adjust to sex with a penile implant. However, many men find that their sex life improves, knowing that they can now count on having a firm erection. Men who have problems with their device or have further questions should talk to their doctor.
Resources
Cleveland Clinic
“Penile Implants” (Last reviewed: November 11, 2022) https://my.clevelandclinic.org/health/treatments/10054-surgical-penile-implants
EAU Patient Information (European Association of Urology)
“What to Know about Penile Implants with Dr. Melissa Mendez” (Urology Care Podcast. 2021) https://www.urologyhealth.org/healthy-living/urology-care-podcast/sexual-health-podcasts/what-to-know-about-penile-implants-with-dr-melissa-mendez
Sexual Supplements: What Patients Should Know
Can a supplement improve a person’s sex life?
Looking at store shelves and media advertising, one might think so. Around the world, people spend millions of dollars on dietary supplements each year. Many of the products are advertised as sexual enhancement products, claiming to boost libido, increase sexual pleasure, or give a man firmer erections.
Supplements are attractive for many reasons. For one, they’re discreet. A man searching for solutions for erection problems might order a supplement online, and nobody has to know he’s seeking help. For another, they’re easy to find in drugstores, convenience stores, and health food stores. And third, people think they might find a solution to a problem and can avoid discussing such a personal issue with another person, even if it is a doctor.
However, consumers need to approach these products with a great deal of skepticism. They often do not live up to manufacturers’ claims, and some can be dangerous.
Below are some things to think about before taking a sexual enhancement supplement.
Supplement ingredients
Sexual enhancement supplements may contain ingredients like the following:
Tribulus terrestris
Ginseng
Maca
Fenugreek
Horny goat weed
Arginine
Zinc
Yohimbine (sometimes called yohimbe)
Vitamin B6
Vitamin B9 (folate)
Vitamin D
Consumers need to approach these products with a great deal of skepticism. They often do not live up to manufacturers’ claims, and some can be dangerous.
FDA doesn’t test or approve dietary supplements
Unlike drugs, dietary supplements do not go through a testing or approval process with the U.S. Food and Drug Administration (FDA). In addition, manufacturers are not required to give the FDA any backup to their safety claims.
The supplement may not be as effective as claimed
Are sexual enhancement supplements effective? This is a difficult question to answer, as the sexual effects of these substances may not be widely studied—at least not in humans. For example, in a 2019 Journal of Sexual Medicine paper, researchers examined 413 studies on sexual enhancement supplements. Only 17% of the studies involved humans.
claims on effectiveness may not be backed up by scientific study, and positive reviews might not be truthful.
Lack of peer-reviewed study—or any kind of study in humans—raises questions as to whether supplements are as effective as their manufacturers claim.
Product reviews are another concern. When researching supplements online, consumers may see vast praise from reviewers, with claims like “It completely cured my erection problems!” or “Sex is better than ever!” However, the internet is rife with unreliable reviews. Some companies pay reviewers to give positive reviews, even if the reviewer did not have a positive experience (or any experience) with the product.
In the above study, researchers used review analysis software to filter out reviews that met the criteria for being unreliable. Once the questionable reviews were removed from the analysis, positive claims dramatically fell. The authors wrote:
After filtration, we observed a 77% decrease in reviews reporting improved erection strength, an 83% decrease in reviews reporting improved ability to maintain erection, a 90% decrease in reviews reporting increased sexual satisfaction, an 88% decrease in reviews reporting increased enjoyment with intercourse, and an 89% decrease in reviews reporting increased erection confidence.
In short, claims on effectiveness may not be backed up by scientific study, and positive reviews might not be truthful.
Products may include hidden ingredients, which could be dangerous.
Supplements may include ingredients that are not listed on the package label. (These are called undeclared ingredients.) There have been cases where sexual enhancement supplements have included erectile dysfunction drugs like sildenafil and tadalafil. These drugs are effective for many men, but not all men can take them safely. They can be especially dangerous for men who take nitrates. But if the ingredients are not declared, it’s difficult for people to know if a product contains substances that could harm them.
Sex problems may be related to another health issue, which could be dangerous.
A sexual problem is often a sign of an underlying medical condition. And often, treating that underlying condition solves the problem.
For example, erectile dysfunction can be an early symptom of diabetes or heart disease. It’s also common in men with obesity. For many men, taking steps to control blood sugar, blood pressure, weight, and other health issues leads to better erections—and better sex.
Seeing a doctor for a sexual issue can help solve the problem and lower the risk of having other health issues, and perhaps avoid a major health crisis, in the future. It’s a win-win situation.
Also, adopting healthy habits can go a long way in improving erections—and sex in general. Many people feel more energetic, confident, and attractive when they take good care of their health.
Take action
When faced with a sexual problem, trying a supplement may seem like an easy plan to try. But it’s important to do some homework first:
See a doctor. Sexual issues are common, and one of the best ways to start addressing them is getting a full check up with a doctor. If another health condition, like diabetes or heart disease, is causing the sexual issues, then it’s important to treat that. (Sexual problems often improve when the underlying cause is treated.)
Ask a doctor or pharmacist about the supplement. These experts can provide information on the safety of a product’s ingredients and what side effects may occur. They can also answer any questions.
Read the supplement label and packaging insert. If anything looks amiss, the manufacturer should be able to give more information.
Check the FDA’s list of tainted sexual enhancement products. The FDA maintains a public list of supplements that could be risky.
With good information, people can make informed decisions. And the best information for a person’s individual situation comes directly from their doctor, not from a supplement manufacturer that doesn’t know the consumer and might not have patients’ best interests at heart.
Sex can be a sensitive topic for any couple. Some people are shy about their bodies or feel embarrassed discussing a subject so private and personal. But there are times when sexual issues need attention, and Peyronie’s disease can be one of those times.
Peyronie’s disease can make intercourse difficult—and sometimes impossible. Plaques (scar tissue) form just beneath the skin of the penis, which becomes less flexible. As a result, the penis starts to bend. The extent of the curvature varies, but it can be as high as 90 degrees.
If there are lots of plaques, the penis might take on an hourglass shape. It could also narrow at the tip (a “bottleneck” deformity) or at the base (a “cobra head” deformity). For some men, there is a “hinge” effect that could make the penis unstable during an erection
Peyronie’s disease can be painful, too. And some men develop erectile dysfunction. They may have sex less often or stop having sex altogether.
There’s an emotional component to Peyronie’s disease as well. Men may feel ashamed of the way their penis looks, have doubts about their masculinity, and worry that their partner will think they’re less attractive. They may also feel anxious about their partner’s sexual satisfaction and fear changes in the relationship. Depression is common, as many men miss the robust sex life they once enjoyed.
And Peyronie’s disease impacts partners. They often notice that the relationship has changed and miss what used to be. If the man with Peyronie’s withdraws, partners may feel isolated or neglected.
Fortunately, like many sexual problems, Peyronie’s disease can be treated in several ways. The process starts with a conversation. And good communication between partners can make treatment more successful.
Broaching the subject
Couples might start the conversation when they’re alone and feeling relaxed. Here are some sample openings:
There’s something that’s been on my mind lately—something sexual—and I was hoping we could talk about it.
I really enjoy our intimate times together, but there’s something troubling me. Can we talk?
It’s okay to admit to feeling nervous or awkward. Often, the subject has been on the partner’s mind, too, but they haven’t been sure how to approach it. Starting the dialogue might bring a sense of relief.
Opening up
Peyronie’s disease comes with a range of emotions, and it’s good to get those out in a constructive way. Frustration, depression, fear, anxiety—they’re all valid. When such feelings are out in the open, couples gain some perspective. They can listen to each other, reassure each other, and approach the future together, as a team.
Keeping the conversation going
Talking about Peyronie’s disease doesn’t need to be a “one and done” conversation. Over time, and as treatment progresses, feelings and perceptions might change. Checking in with each other from time to time can enhance the overall dialogue.
Learning together
Peyronie’s disease isn’t a term people hear every day. For some, it might be brand new. Researching the topic together is another way to keep the conversation going. Some couples share what they discover online, on television, or in magazines. They might also attend doctor’s appointments together and ask questions.
Exploring together
Peyronie’s disease doesn’t have to stop a couple from being intimate, and sex is more than intercourse. Couples can focus on what is possible and enjoyable. This part of the conversation can be creative and fun.
Staying supportive
Encouragement is important for couples facing Peyronie’s disease, and each partner can be a cheering section of sorts. For example, after a man finishes a round of treatment, a partner might say, “That couldn’t have been easy. I’m proud of you!” Or if a man has trouble keeping an erection during a sexual encounter, the partner might say, “That’s okay. I love what we do together.”
Considering counseling
Even when they have the best of intentions, couples may still struggle with communication. This is when a couples counselor might help. A trained therapist can teach strategies for expressing thoughts clearly, listening respectfully, and responding constructively. Urologists can make referrals for therapy.
For single men
For single men with Peyronie’s disease, starting new sexual relationships can be especially daunting. If they are still getting to know a new partner, they may be unsure of what to disclose and when.
Much of the advice above can apply to single relationships. Building trust takes time, but couples just starting out can still have similar conversations about Peyronie’s disease and its effects on intimacy.
A man might say, “Before we take the relationship further, there’s something I want to talk to you about.” If the relationship has been supportive and based on trust up to this point, chances are the partner will respond positively and be open to discussing other options for intimacy while the man seeks treatment.
Wrapping up
Sometimes the hardest part of having a sexual discussion is starting it. But all it takes is a deep breath. It may not be perfect or go exactly as planned, but starting the conversation is usually better than not having it at all.
Having a vasectomy is a step that should be carefully considered because it’s a permanent form of birth control. (It’s true that vasectomies can be reversed, but doing so requires a second, more involved procedure.) The following Q&A goes over many of the questions many men have as they’re contemplating having a vasectomy.
What happens during a vasectomy?
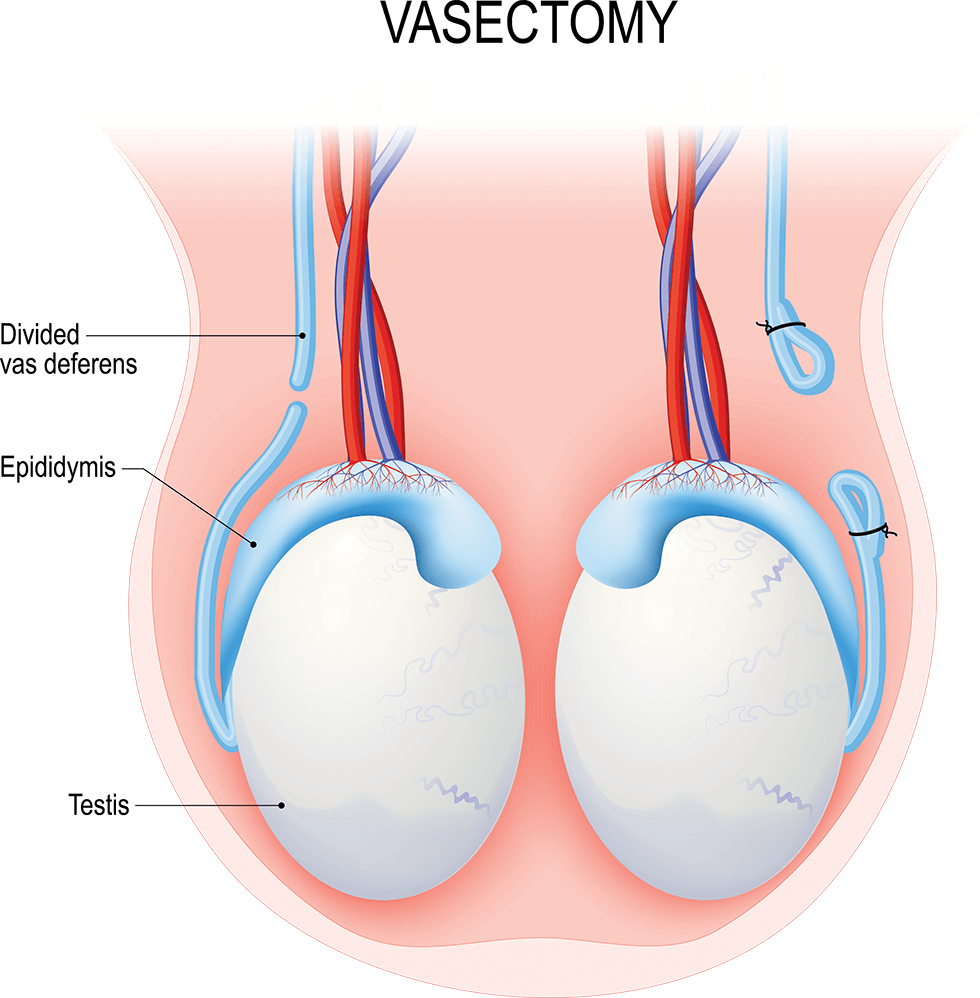
A vasectomy is a simple surgical procedure done to prevent pregnancy. It involves cutting two tiny tubes called the vasa deferentia. (One tube is called a vas deferens or vas.)
Typically, sperm cells travel through the vasa deferentia before they’re mixed with semen and ejaculated out of the body. By cutting these tubes, the sperm cells’ path is blocked. Instead of being ejaculated, the cells are absorbed by the man’s body.
What is a conventional vasectomy?
During a conventional vasectomy, the surgeon accesses the vasa deferentia through one or two small incisions in the scrotum, the sac that holds the testicles. After the vasectomy is done, the scrotal incisions are closed with dissolvable stitches.
What is a no-scalpel vasectomy?
With a no-scalpel vasectomy, the puncture heals on its own, and no stitches are necessary.
With a no-scalpel vasectomy, the surgeon accesses the vasa deferentia through a tiny puncture made in the scrotum. The puncture heals on its own, and no stitches are necessary.
How effective is a vasectomy?
After it takes effect, a vasectomy is about 99.95% effective in preventing pregnancy. This success rate makes it the second most effective form of birth control available. (The first is abstinence—not having sex at all.)
Where are vasectomy procedures done? How long do they take?
Most vasectomy procedures can be done in a urologist’s office. Occasionally, they may be done at a surgical center or hospital. They take about a half hour, and men can go home the same day.
Is a vasectomy covered by health insurance? How much does it cost?
Vasectomies are often covered by health insurance in the United States. A man should check with his insurance company for details on his specific coverage and his out-of-pocket costs. Costs can vary depending on location and the type of surgery needed.
Does it hurt to have a vasectomy?
Men are given local anesthesia (the area is numbed), so there shouldn’t be any pain. There might be some minimal discomfort after the anesthesia wears off. This can usually be managed with ice packs (placed over clothing) or acetaminophen (Tylenol). Aspirin or ibuprofen are not recommended, as they raise the risk of bleeding or bruising.
Can there be complications after a vasectomy?
All surgical procedures have some risk, but complications after a vasectomy are rare. In fact, the American Urological Association notes that complication rates are around 1% to 2%. Complications can include the following:
Sperm granuloma. When a vas deferens is cut, stray sperm cells can leak out. The immune system responds, which can lead to inflammation and, eventually, a small mass called a sperm granuloma. The mass is benign (not cancerous). A sperm granuloma can cause some temporary discomfort, but it usually goes away on its own. Pain medications may help. If it is especially bothersome, it may need to be surgically removed.
Infections. Some men develop an infection after their vasectomy. The infection is usually treated with antibiotics.
Hematoma. A hematoma occurs when blood collects in the scrotum after surgery. It often goes away on its own, but men should call their doctor if their scrotum gets bigger or becomes painful.
Post-vasectomy pain syndrome. About 1% to 2% of men have chronic pain after vasectomy due to fluid buildup in the scrotum. Pain medications and warm baths may help. In more severe cases, surgery—or a vasectomy reversal procedure—may be needed.
Research shows that men who have vasectomies are not at higher risk for cancer or ED.
No. Research shows that men who have vasectomies are not at higher risk for cancer or ED.
What is the vasectomy recovery period like?
Most men take it easy for a day or two after their vasectomy. There may be some pain and swelling, but these symptoms can be managed with pain medication and cold packs.
Men who work desk jobs usually go back to work the next day. Heavy lifting is restricted for about a week, so men with more physically demanding jobs may need to adjust their routine.
Men should avoid ejaculation—through partnered sex or masturbation—for about a week.
Is a vasectomy effective immediately?
No. It takes time for sperm cells to “clear” each vas deferens after a vasectomy. For this reason, couples need to continue using another form of birth control for a few more months or about 20 ejaculations.
After that period, men can see their urologist for a semen analysis. The doctor will check a semen sample for sperm cells. If some remain, couples should continue using birth control for a bit longer. If the semen is clear of sperm, other birth control methods should no longer be needed.
The best way to know whether sperm cells have cleared is to have a semen analysis with a urologist.
What happens to sperm cells after a vasectomy?
Instead of being ejaculated, sperm cells are absorbed by the body. This process is harmless.
What is sex like after a vasectomy?
Sex drive and orgasms feel the same as they did before the procedure. Semen volume should also be about the same, as sperm makes up a small percentage. Partners don’t feel a difference either.
Some men find sex to be more exciting after a vasectomy because they can be more spontaneous. The anxiety of unwanted pregnancy is reduced.
Does a vasectomy protect against sexually transmitted infections?
No. While vasectomies are extremely effective in preventing pregnancy, they do not protect against sexually transmitted infections (STIs) like HIV, HPV, and gonorrhea. Couples should still practice safe sex by using condoms and/or dental dams. Regular testing for STIs may also reduce the risk of transmission.
Can a vasectomy be reversed?
Yes. In general, vasectomy is considered a permanent decision, and men should think carefully before having one. But there are times when a man decides he would like to father children after all. That’s when a vasectomy reversal may be considered.
A vasectomy reversal procedure reconnects the ends of the vasa deferentia, giving sperm cells a clear path out of the body. (In some cases, the end of a vas may need to be connected to the epididymis, a coiled tube that links a testis with a vas deferens. The epididymis stores sperm cells.)
Vasectomy reversals are more involved than vasectomies, and they don’t always lead to pregnancy. Success can depend on how much time has passed between the vasectomy itself and the reversal. The longer the time frame, the less likely a pregnancy will happen.
It also takes time—sometimes a few months to a year—before sperm cells reappear in the semen.
Other factors, including a man’s overall health and the health and age of his partner, play a role in getting pregnant, too.
Besides vasectomy reversal, are there other ways to become a biological father after having a vasectomy?
Yes. It might be possible to retrieve sperm cells from the testes. These cells can then be used for in vitro fertilization (IVF).
Some men have their sperm frozen and stored by a sperm bank before their vasectomy, just in case they change their mind about fatherhood later.
“You are what you eat” has been a popular phrase in English for decades. And it makes sense. Much of a person’s overall health is linked to their eating habits. A balanced, nutritious diet can lower risk for a variety of health conditions, like heart disease and diabetes. And a diet full of fast food and TV dinners could have the opposite effect.
Scientists have studied the way a man’s eating habits may affect his ability to get erections. Not surprisingly, men with healthier diets often fare better.
This notion applies to sexual health, too. For example, scientists have studied the way a man’s eating habits may affect his ability to get erections. Not surprisingly, men with healthier diets often fare better.
So what should men eat? While choosing healthy foods is wise, researchers have found that the Mediterranean diet could be an easy, effective path to better erections in the future.
For example, a 2020 JAMA Network Open study investigated the link between diet and erections in over 21,000 men aged 40 to 75 living in the United States. The researchers discovered that men who followed a Mediterranean or similar diet were less likely to have erectile dysfunction (ED) compared to those who didn’t.
And in 2021, researchers presented preliminary results on this topic at the European Society of Cardiology’s annual meeting. After reviewing data from 250 men with high blood pressure and ED, they reported that the Mediterranean diet could be linked to better erectile function.
What is a Mediterranean Diet?
A Mediterranean diet is widely eaten in countries around the Mediterranean Sea, such as Spain, Italy, and Greece.
A Mediterranean diet is widely eaten in countries around the Mediterranean Sea, such as Spain, Italy, and Greece. Because it encompasses a variety of cultures, there’s no one “official” Mediterranean diet. But diets in this geographic area have some similarities:
More plant-based foods. Fruits, vegetables, whole grains, nuts, and legumes (like beans and chickpeas) are staples of a Mediterranean diet.
Limited red meat, eggs, and dairy. Red meat is seldom eaten on a Mediterranean diet. Eggs and butter are used sparingly.
Moderate amounts of lean meats. Mediterranean diet followers eat poultry, like chicken and turkey, every once in a while.
More seafood. Fish and shellfish—such as salmon, tuna, and clams—might be eaten several times a week.
Healthy fats. Monounsaturated fats, like olive oil and avocados, are favored over saturated fats and trans fats, which are found in items like red meat, cakes, cookies, and processed foods.
Fewer desserts. Sweets and traditional desserts are eaten in moderation. Fruit is a frequent dessert substitute.
Alcohol. Alcoholic beverages, such as red wine, are included in a Mediterranean diet, but only if safe to do so. People should avoid alcohol if they are pregnant, tend to misuse alcohol, or have a health condition that worsens with alcohol use.
Fewer processed foods. Following a Mediterranean diet often means preparing meals from fresh, basic ingredients rather than relying on processed foods.
Mediterranean Diet and ED: What’s The Connection?
How might a Mediterranean diet help with a man’s erections?
It’s good for the cardiovascular system
This system includes the heart and the roughly 60,000 miles of blood vessels throughout the body. Some of these blood vessels are in the penis. Because a firm erection depends on blood flow, these blood vessels need to be clear.
Research suggests that the Mediterranean diet keeps the lining of blood vessels healthy and reduces the risk of atherosclerosis (hardening of the arteries), which can interfere with blood flow. With the path open, blood can flow to the penis—and form an erection—more easily.
It helps with the production of nitric oxide
This chemical plays an important role in erections. Before blood can flow into the penis for an erection, the arteries need to relax and dilate. Nitric oxide is essential for this process.
It lowers a man’s risk for diabetes
Men with diabetes are at higher risk for ED than men without diabetes. They also tend to get ED several years earlier.
High blood sugar can damage blood vessels and nerves. As noted above, blood vessel damage can limit blood flow into the penis. And nerve damage can interfere with signals from the brain that “tell” the penis to start an erection when a man is sexually aroused.
It helps with weight management
The heavier a man is, the higher his risk for ED. A healthy diet, combined with physical activity, can be a good way to manage weight. That said, people still need watch their calories, even with a Mediterranean diet.
Putting it All Together
So can eating a Mediterranean diet prevent ED altogether? Could it cure ED?
Scientists aren’t sure yet, but they’re interested in finding out. For now, research suggests that men who follow a healthier diet could be less likely to develop ED later. But researchers don’t know yet whether diet can prevent ED altogether or whether changing dietary habits can improve ED in men who already have trouble with erections.
The good news, however, is that a healthy diet benefits the body from head to toe. And many people find that taking care of the whole body improves their sexual health as well as their overall wellbeing.
Jimenez-Torres, Jose, et al. “Mediterranean Diet Reduces Atherosclerosis Progression in Coronary Heart Disease: An Analysis of the CORDIOPREV Randomized Controlled Trial” (Originally published: August 10, 2021) https://www.ahajournals.org/doi/full/10.1161/STROKEAHA.120.033214
Prostate Cancer Myths and Popular Beliefs: What’s True and What’s Not True?
Men looking for information on prostate cancer have a lot of information to sift through. And while there is plenty of reliable information out there, there are also quite a few myths and misconceptions swirling around, often spread online through unreliable sources or by word via well-meaning but uninformed people.
But it’s important to know the facts. Prostate cancer is the second most common cancer in men, according to the American Cancer Society. In fact, about 1 in 8 men will be diagnosed with prostate cancer during their lifetime.
The goal of this article is to debunk false information and clarify some of the issues medical scientists still debate. For topics still in debate, we put this information into context using current, peer-reviewed research.
Here are some of the most common questions and areas of debate.
Do vasectomies raise a man’s risk for prostate cancer?
When considering their birth control options, many men choose vasectomy. This surgical procedure is simple, safe, and effective, with an estimated success rate of 99.95%.
For many years, scientists have investigated whether a vasectomy can raise the risk of prostate cancer.
Over the last few years, it has been reported that vasectomies do not cause prostate cancer. The Mayo Clinic reports that “[a]lthough there have been some concerns about a possible link between vasectomy and testicular or prostate cancer in the past, there’s no proven link.”
It’s possible that vasectomy itself might not increase risk, but more prostate cancer cases might be discovered during pre-vasectomy medical exams.
Does frequent ejaculation reduce risk for prostate cancer?
Scientists have studied the relationship between ejaculation frequency and prostate cancer for several years. Some think that ejaculation flushes out harmful substances in the semen that could be linked to prostate cancer.
Research results have been mixed. For example, the authors of a 2018 Journal of Sexual Medicine study found that men who ejaculate 2 to 4 times a week were at lower risk for prostate cancer. But other researchers have reported no association.
Does eating flaxseeds affect prostate cancer risk?
Flaxseeds are a popular dietary supplement. They are thought to help with constipation, diabetes, heart disease, and other conditions. Could prostate cancer be another?
Scientists don’t know for sure. Flaxseeds contain phytoestrogens, which are similar to estrogen, a hormone naturally produced by the body. Some researchers believe that this property might affect the risk of hormone-related cancers, like prostate cancer. Other studies have found that flaxseeds don’t impact prostate cancer risk at all.
Nowadays, the effects of flaxseeds on prostate risk isn’t clear, and scientists continue to study the relationship.
The effects of flaxseeds on prostate risk isn’t clear
However, some experts suggest that men who already have prostate cancer might benefit from flaxseeds, as flaxseeds have been associated with lower PSA levels and decreased tumor aggressiveness. (PSA is a protein made by the prostate. Lower PSA levels suggest that prostate cancer cells are growing more slowly.)
Can pomegranate reduce or slow down prostate cancer growth?
In the past, studies have suggested that drinking pomegranate juice might slow the growth of prostate cancer cells. It was thought that pomegranates contained antioxidants and other substances that might reduce inflammation and lower PSA levels.
However, experts now report that there isn’t enough evidence to support the use of pomegranate for the treatment or prevention of prostate cancer.
Is prostate cancer less dangerous than other types of cancers because it grows more slowly than other types of cancers?
Many men with prostate cancer have a good prognosis, especially if the cancer is caught early and hasn’t spread outside the prostate gland. Prostate cancer tends to grow slowly, and men might not need treatment right away. (In this case, they might opt for active surveillance: Their cancer will be closely monitored, but they won’t receive treatment until they have symptoms or until the cancer becomes more aggressive.)
However, this isn’t the case for all men. The American Cancer Society estimates that 268,490 new cases of prostate cancer will be diagnosed in 2022, and about 34,500 men will die of the disease this year.
So the answer is, “No, it’s not less dangerous.” Men need to follow their doctor’s treatment instructions as prescribed and keep themselves as healthy as they can. Doctors can guide men on healthy lifestyle habits.
Is prostate cancer a disease of older men only? Do young men ever get prostate cancer?
It’s true that prostate cancer is more common in older men. According to the American Cancer Society, about 60% of new prostate cancer cases are diagnosed in men aged 65 or older. The average age at diagnosis is 66. And prostate cancer is rare in men younger than 40.
But that doesn’t mean prostate cancer isn’t possible in younger men. Forty percent of new cases are in men under age 65. And some men have risk factors, such as a family history of prostate cancer, that could make them more vulnerable when they’re younger.
Men who are concerned about their prostate cancer risk should ask their doctor about screening.
Does prostate cancer run in families?
Scientists aren’t certain what, exactly, causes the disease
Prostate cancer can run in families. If a man has a first-degree relative (parent or brother) with prostate cancer, his risk for developing prostate cancer is about 2 to 3 times higher than average. His chances of having prostate cancer go up even higher if he has more than one first-degree relative with prostate cancer and if these relatives were diagnosed at a younger age.
Still, most cases of prostate cancer are not family-related. Scientists aren’t certain what, exactly, causes the disease.
Can an enlarged prostate (aka BPH) lead to prostate cancer?
It is possible for a man to have an enlarged prostate and prostate cancer, even at the same time. But there’s nothing about an enlarged prostate that makes a man more likely to get prostate cancer.
The medical term for an enlarged prostate is benign prostatic hyperplasia (BPH). The word benign is an important one here, as it means there is no cancer present. As a man gets older, his prostate gland usually becomes larger. For some men, this isn’t a problem. But for others, the prostate growth squeezes the urethra (the tube that allows urine to exit the body) and makes urination difficult.
Enlarged prostate and prostate cancer do have similar symptoms, including trouble passing urine. Men who experience these symptoms should see their doctor for a checkup. (Learn more about enlarged prostate treatments.)
Does prostate cancer always have symptoms?
Actually, prostate cancer often has no symptoms, especially in its early stages. That’s why it’s so important to be screened, especially for men with risk factors.
Prostate cancer often has no symptoms
Common symptoms include urination difficulties, painful ejaculation, and blood in the urine or semen. Other urologic conditions, such as prostatitis (inflammation of the prostate), can have these symptoms, too. That’s why doctors do a complete checkup if men have these symptoms.
Is PSA testing reliable for diagnosing prostate cancer? Does having a high PSA level means a man has cancer?
PSA stands for prostate-specific antigen, a protein produced by the prostate. It is used to screen for prostate cancer, but it is not the only test that is used.
Having high levels of PSA could mean that a man has prostate cancer. But it could mean other things as well. For example, men with prostatitis or an enlarged prostate (benign prostatic hyperplasia or BPH) may also have elevated PSA levels.
If a man’s PSA screening shows high PSA levels, his doctor will consider his health history, symptoms, and the results of other tests (such as a digital rectal exam) to decide how to proceed. If prostate cancer is suspected, a biopsy may be done. During a biopsy, a small portion of prostate tissue is removed and examined for cancer cells.
Does having a prostate biopsy cause cancer to spread? Can prostate cancer cells “break off” during a biopsy?
If a doctor suspects prostate cancer due to a man’s symptoms, family history, etc., a prostate biopsy is usually the next step in evaluation. During a biopsy, a surgeon removes a small piece of tissue. A pathologist examines the sample under a microscope. If cancer cells are found, doctors use biopsy information to determine the stage and grade of the cancer and develop a personalized treatment plan.
Some patients worry that cancer cells can break off and spread during the biopsy procedure.
While there have been case reports of this happening, it is quite rare. The benefits of having a biopsy far outweigh the risk of cancer cells spreading during the procedure.
Does prostate cancer always require surgery?
Radical prostatectomy — the surgical removal of the prostate gland — is a common prostate cancer treatment.
But not all men with prostate cancer have surgery. For example, radiation, chemotherapy, and hormonal therapy are other treatment options.
In some cases, the cancer doesn’t need to be treated right away. As mentioned above, some men may choose active surveillance. If their cancer doesn’t appear to be aggressive, they may hold off on any treatment. At that point, a healthcare professional regularly monitors their cancer’s progress, and treatment begins only when necessary.
When recommending prostate cancer treatment, specialists consider many factors, including the stage and risk level of the cancer and the patient’s age, overall health, and treatment preferences.
Note: Another surgical option is orchiectomy — removal of the testicles. These organs produce testosterone, a hormone that helps prostate cancer cells grow. Removing the testicles greatly reduces the amount of testosterone available to cancer cells.
Can prostate cancer negatively affect a man’s sex life? Do men still enjoy sex after prostate cancer treatment?
Sexuality is a big concern for men with prostate cancer, and rightly so. Certain treatments, such as surgery to remove the prostate gland (radical prostatectomy), can damage the nerves responsible for erections. This can lead to erectile dysfunction (ED). Treatments might also change the way that ejaculation and orgasms feel.
Fortunately, there are treatments available for ED and other sexual issues. It may take some time and adjustments, but men can still enjoy sex after prostate cancer.
Does prostate cancer impact a man’s fertility?
Prostate cancer treatment may make it more difficult for a man to father a child. Some men have their testicles removed as part of prostate cancer treatment, and without these organs, they cannot produce sperm. If the prostate and seminal vesicles are removed, there will be no prostatic fluid produced to protect sperm cells.
Radiation and chemotherapy can affect the production of sperm and prostatic fluid, too.
Some men bank their sperm before their treatment begins. With this method, their sperm is frozen and used later for in vitro fertilization. It may also be possible to extract sperm from the testicles, if they haven’t been removed.